
Exercise After BBL : Quick Summary
Most patients begin light walking within 24 hours of BBL surgery and receive clearance for low-impact cardio at 4-6 weeks. Full gym workouts, including lower body resistance training, typically resume at 10-12 weeks.
When Can You Exercise After a BBL?
Light walking starts within 24 hours of surgery. Low-impact cardio clears at 4-6 weeks. Full gym training, including squats and lower body resistance work, is permitted at 10-12 weeks post-operatively.
Light walking begins within 24 hours of BBL surgery to prevent blood clots and support fat graft survival. Low-impact cardio receives clearance at 4-6 weeks post-operatively. Full lower body resistance training typically returns at 10-12 weeks, once fat grafts have established a stable blood supply in surrounding tissue.
Published research indicates that 20-40% of transferred fat is reabsorbed in the first 6 weeks. Exercising too soon during this window is the leading cause of diminished BBL volume. For patients travelling from the UK or USA to Istanbul, flying clearance is typically granted at 2-3 weeks with compression stockings.
Why Trust This Guide
This guide draws on ISAPS global outcome data, BAAPS post-operative guidance, and peer-reviewed research published in Plastic and Reconstructive Surgery journal.
It is medically reviewed by Op. Dr. Alirza Jahangirov, Plastic, Reconstructive & Aesthetic Surgeon at Carely Clinic in Istanbul, with experience in BBL and body contouring procedures.
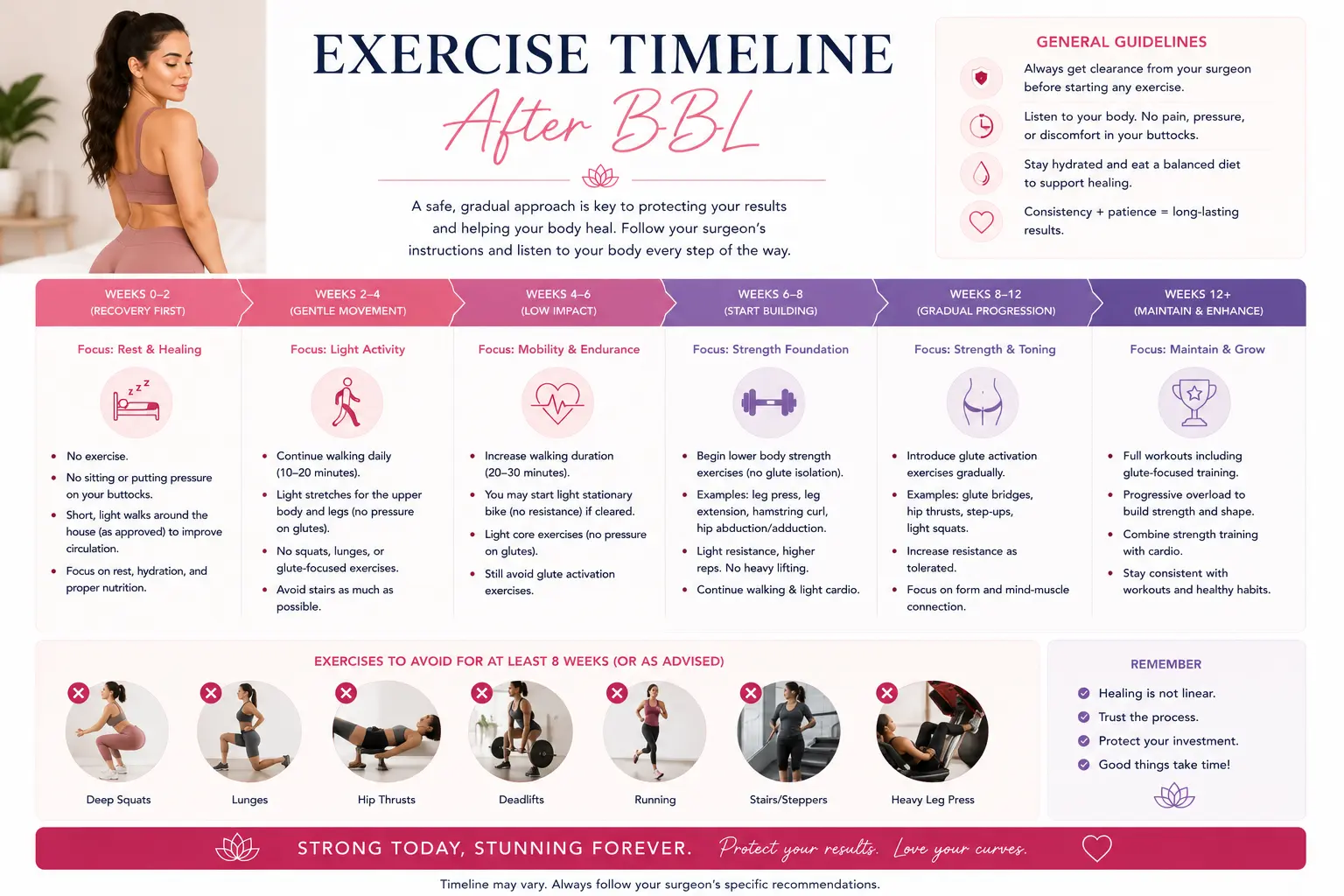
Week-by-Week BBL Exercise Timeline
The BBL exercise timeline runs from day-1 walking to full gym training at week 12. Each phase protects fat graft vascularisation while maintaining circulation and preventing complications.
The recovery timeline below applies to standard BBL procedures. Patients who combine BBL with liposuction in multiple donor areas may require a modified schedule — confirm with your surgeon at each follow-up.
Weeks 1-2: Walking Only
In the first two weeks, only light walking is permitted. Short 5-10 minute walks every 2-3 hours are actively encouraged from the day after surgery, as early ambulation significantly reduces DVT risk in post-surgical patients. All other exercise — including yoga, stretching, and upper body training — is restricted.
No sitting directly on the buttocks. Sleep on your stomach or side. Wear your compression garment continuously except when showering.
Weeks 3-4: Gentle Mobility
Gentle mobility work and extended daily walking resume in weeks 3-4. Standing hip circles, light ankle rotations, and upper body mobility are permitted. No loaded movements, no machines, and no exercise requiring a seated position. Most patients can manage 20-30 minute walks at a comfortable pace by week 4.
Weeks 5-6: Low-Impact Cardio
Low-impact cardio is typically cleared at the 4-6 week mark after surgeon confirmation. Brisk walking outdoors, stationary cycling at low resistance, and elliptical training at moderate pace are appropriate. Most surgeons recommend keeping heart rate below 120 bpm throughout this phase to prevent excessive metabolic pressure on fat grafts.
Weeks 7-8: Moderate Activity
Upper body resistance training returns at weeks 7-8 for most patients. Dumbbell and cable exercises targeting the shoulders, chest, back, and arms are permitted, provided no sitting or lying directly on the gluteal region is involved. Continue avoiding squats, lunges, leg press, and any glute-specific loading.
Weeks 9-12: Strength Training Returns
Gradual lower body training begins at weeks 9-12 under explicit surgeon clearance. Start at 50% of your pre-surgery capacity. Introduce bodyweight squats before progressing to loaded movements. Avoid exercises requiring direct seated glute pressure — including leg press machines and cable pull-throughs performed from a bench.
Beyond 12 Weeks: Full Activity
Full gym activity, including HIIT and heavy compound lifts, resumes after the 12-week mark. Published research indicates that approximately 60% of transferred fat cells have established permanent blood supply by the 3-month mark, making this the threshold for unrestricted training. Always seek a formal sign-off from your surgeon at the 12-week follow-up before returning to high-intensity training.
| Week | Permitted Activity | Still Restricted |
|---|---|---|
| Days 1-14 | Short light walks (5-10 min), ankle rotations | All exercise, sitting on buttocks, sleeping on back |
| Weeks 3-4 | Extended walks (20-30 min), standing upper body mobility | Loaded exercise, seated equipment, strenuous activity |
| Weeks 5-6 | Stationary cycling, elliptical (HR below 120 bpm), brisk walking | Running, HIIT, squats, lunges, lower body resistance |
| Weeks 7-8 | Upper body weights (shoulders, chest, back, arms) | Squats, lunges, leg press, glute isolation, running |
| Weeks 9-12 | Bodyweight squats, light lower body training, jogging | Heavy compound lifts, HIIT, direct seated glute load |
| 12+ Weeks | Full gym activity with surgeon sign-off | None — all activity permitted |
5 Factors That Affect Your Return-to-Exercise Timeline
Individual recovery speed depends on five key variables — procedure complexity, age, donor site volume, pre-surgery fitness level, and adherence to post-operative protocols. No two BBL recoveries are identical.
The 12-week timeline above represents the standard pathway for uncomplicated BBL procedures. These five factors can extend or occasionally accelerate your personal schedule:
- Procedure complexity. Patients undergoing BBL combined with tummy tuck or multiple-area liposuction typically require an additional 2-4 weeks before resuming cardio, as the body is recovering across multiple surgical sites simultaneously.
- Age. Patients over 45 generally experience slower fat graft vascularisation than younger patients, in line with general clinical observation on age and tissue healing. Cardio clearance may shift to 6-8 weeks rather than 4-6.
- Volume of fat transferred. Higher-volume transfers of 600ml or more per side require a longer compression period and stricter sitting restrictions, delaying exercise clearance by 1-2 weeks.
- Pre-surgery fitness level. Highly active patients report faster functional recovery, but this does not equate to earlier surgical clearance. Fat graft survival depends on vascularisation, not cardiovascular fitness.
- Adherence to compression garment use. Wearing your compression garment for the full prescribed 6-8 weeks reduces swelling and supports fat integration, directly influencing when your surgeon will clear you for gym activity.
Expert Insight
“Patients who maintain compression garment use continuously for the full 8 weeks and attend all follow-up appointments consistently receive earlier exercise clearance than those who don’t. Compliance is the single most controllable factor in your timeline.”
— Reflecting current clinical practice on BBL recovery and compliance
Exercises to Avoid After BBL (and Why)
Squats, lunges, running, HIIT, and any seated machine work are restricted for 8-12 weeks post-BBL because they compress or destabilise fat grafts before permanent vascularisation is complete.
Fat Graft Survival Window
The 6-week post-surgery window is when fat grafts are most vulnerable. During this period, transferred fat cells are developing a new blood supply in the gluteal tissue. Direct mechanical pressure, elevated heart rate, or rapid movement disrupts this process and causes cell death.
Published research consistently links high-impact exercise before 8 weeks to measurably reduced fat retention outcomes. Plastic surgery clinical consensus is that premature glute loading compresses fat cells before vascularisation is complete.
Lower Body Exercises to Avoid
For the first 8-10 weeks, avoid all of the following:
- Squats and lunges — direct compressive load on gluteal tissue
- Leg press and hack squat — seated glute pressure combined with resistance loading
- Running, jumping, and plyometrics — high-impact ground reaction forces transmitted through the gluteal region
- HIIT training — combines high impact with calorie deficit risk
- Hip thrusts and glute bridges — isolated glute loading too early risks fat displacement
Upper Body and Cardio Restrictions
- Seated rowing machines — avoided until 8 weeks due to seated gluteal pressure
- Spin classes — permitted from week 5 only with a specific padded seat and low resistance; confirm with your surgeon
- Flat bench press — lying on the back is restricted for most patients until weeks 6-8; use an incline bench alternative
Safe Exercises After BBL: What You Can Do and When
Light walking from day 1, upper body resistance training from week 7, and glute-building exercises from week 12 allow you to stay active throughout recovery without compromising fat graft survival.
Safe Upper Body Work
Standing upper body resistance training is safe from weeks 7-8 onward. Cable rows, standing shoulder press, dumbbell curls, tricep pushdowns, and lateral raises are all appropriate. Ensure all exercises are performed standing or supported by a back pad — never from a flat bench or seated position.
You can read more about recovery planning for combined procedures on the BBL recovery guide and the main BBL Turkey procedure page.
Safe Cardio Options
From weeks 5-6, low-impact cardio options include brisk outdoor walking, stationary cycling at low resistance, and elliptical training. Keep sessions to 20-30 minutes initially and monitor for swelling in the donor areas after each session. If liposuction donor sites show increased swelling post-cardio, reduce intensity and notify your surgical team.
Nutrition and Weight Stability: Protecting Your Fat Grafts
Fat graft survival depends not just on activity restrictions but on maintaining calorie intake. A calorie deficit during recovery metabolises transferred fat, reducing BBL volume and altering contour.
Weight stability is as important as the exercise restrictions themselves. Long-term outcome data consistently shows that patients who maintain weight within 4-6 kg of their surgery weight report substantially higher satisfaction at long-term follow-up compared to those with significant weight fluctuation.
During the first 8 weeks, consume a minimum of 2,000 calories daily. Prioritise lean protein (chicken, fish, eggs), healthy fats (avocado, nuts, olive oil), and complex carbohydrates. Adequate protein intake supports wound healing and fat cell integration.
Once you resume cardio at weeks 5-6, increase your calorie intake proportionally. A 30-minute stationary cycle session burns approximately 200-350 kcal. Failing to replace these calories places fat grafts at risk of metabolic reabsorption.
Clinical observation indicates that a common reason patients present with suboptimal BBL volume at the 3-month mark is not exercise timing — it is sustained calorie restriction combined with cardio resumption. Patients who resume fitness at 6 weeks without adjusting their nutrition often lose more transferred volume than those who fuel their recovery correctly.
Warning Signs to Watch For
Contact your surgeon or an emergency service immediately if you experience any of the warning signs below. Early detection of complications after BBL protects both your health and your results.
Most BBL recoveries are uneventful, but complications do occur and require rapid response. If you are returning home to the UK or US after surgery in Istanbul, save your surgical team’s WhatsApp number and your local emergency contact before you travel.
| Warning Sign | What It May Indicate | Action Required |
|---|---|---|
| Fever above 38.5°C (101.3°F) | Surgical site infection or systemic infection | Contact surgeon immediately; attend nearest A&E or ER if over 39°C |
| Shortness of breath or chest pain | Pulmonary embolism (fat embolism or DVT) | Call 999 (UK) or 911 (US) immediately. Do not wait. |
| Sudden increase in pain after days 3-5 | Haematoma, seroma, or deep infection | Contact surgical team within 2 hours; photograph the area |
| Wound separation or open incision | Wound dehiscence requiring closure | Cover with sterile dressing; contact surgeon same day |
| Hot, swollen, or red calf | Deep vein thrombosis (DVT) | Seek emergency care immediately; do not massage the area |
| Firm, enlarging fluid-filled swelling | Seroma (fluid accumulation) requiring drainage | Contact surgeon for assessment; do not attempt to drain yourself |
| Foul-smelling discharge from incision site | Localised infection requiring antibiotic treatment | Contact surgeon within 24 hours; send a photograph via WhatsApp |
Who Is NOT a Good Candidate for BBL?
BBL is contraindicated in patients with insufficient donor fat, active infection, uncontrolled diabetes, or a BMI below 22. Relative contraindications include smoking history and immune-compromising medication.
Absolute Contraindications
These patients cannot safely undergo BBL under any circumstances:
- Insufficient donor fat (BMI below 22). The procedure requires adequate fat reserves in the abdomen, flanks, or thighs for harvesting via liposuction. Patients with low body fat have insufficient donor volume for meaningful augmentation. Most surgeons require a BMI of at least 22-24 with identifiable donor sites as the minimum threshold.
- Active systemic infection or localised skin infection. Surgery cannot proceed with any active bacterial or viral infection. Standard surgical practice requires patients to be infection-free for a minimum of 4 weeks before scheduling.
- Uncontrolled clotting disorders. Patients with unmanaged coagulation conditions face significantly elevated DVT and haematoma risk. Anticoagulation status must be assessed and optimised before any consideration of BBL surgery.
Relative Contraindications
These patients may qualify after medical optimisation:
- Active smoking. Nicotine reduces blood supply to fat grafts and significantly impairs wound healing. Most surgeons require patients to stop smoking a minimum of 6 weeks before surgery and refrain throughout the 12-week recovery. Nicotine replacement therapy does not exempt a patient from this restriction.
- BMI above 32. Higher BMI patients face elevated anaesthetic and DVT risk. Many surgeons require weight reduction to a BMI of 28-30 before scheduling. This also improves donor fat quality for grafting.
- Autoimmune conditions or immunosuppressant medication. Conditions such as rheumatoid arthritis or lupus treated with immunosuppressants impair healing and fat integration. Medical clearance from a rheumatologist is required before proceeding.
Managing Expectations
Results depend on fat survival, not the volume transferred. Published research indicates that 20-40% of transferred fat reabsorbs during the first 6 weeks regardless of technique. Final results — and therefore final shape — are only visible at the 3-6 month mark. Patients should view pre-operative photos with surgeons and understand that immediate post-surgery shape is not final shape.
Frequently Asked Questions
When can I start working out after a BBL?
Most patients begin light walking within 24 hours and receive full gym clearance at 10-12 weeks. Published research indicates that early high-impact activity in the first 6 weeks reduces fat graft survival rates measurably. Always obtain written clearance from your surgeon before returning to any structured exercise programme.
Can I walk after BBL surgery?
Yes, short light walks are encouraged within 24 hours of BBL surgery to prevent blood clots. Early ambulation significantly reduces the risk of deep vein thrombosis in post-surgical patients. Keep initial walks to 5-10 minutes every few hours; avoid any pace or incline causing discomfort.
When can I do squats after a BBL?
Squats and lunges are typically cleared at the 10-12 week mark, once fat grafts are permanently integrated. Plastic surgery clinical consensus is that premature glute loading compresses fat cells before vascularisation is complete. Reintroduce squats at 50% bodyweight capacity and increase load progressively over 4-6 weeks under surgeon guidance.
What exercises should I avoid after BBL?
Avoid squats, lunges, running, HIIT, and any exercise requiring direct glute pressure for the first 8-10 weeks. Published research linkshigh-impact exercise before 8 weeks to measurably reduced fat retention outcomes. Seated machine exercises and rowing should also be avoided because they place direct pressure on the grafted tissue.
How long after BBL can I sit normally?
Most surgeons clear patients to sit normally without a BBL pillow at 6-8 weeks post-operatively. Most surgeons recommend using a BBL cushion for all seated activities during the first 6 weeks. Short car journeys are permitted from week 3 using a BBL pillow, with longer seated periods reintroduced gradually.
Will running ruin my BBL results?
Running before 8-10 weeks post-BBL significantly increases the risk of fat cell displacement and volume loss.Sustained cardio creates a calorie deficit that may cause the body to metabolise the transferred fat cells. After full clearance, moderate running paired with adequate calorie intake does not compromise established BBL results.
When can I do cardio after a BBL?
Low-impact cardio such as brisk walking and stationary cycling is typically permitted at 4-6 weeks after BBL. Most surgeons recommend keeping heart rate below 120 bpm during this early cardio phase. High-impact cardio including running, jumping, and HIIT training should wait until 10-12 weeks post-operatively.
Can I go to the gym 6 weeks after BBL?
At 6 weeks, most patients receive clearance for upper body training and low-impact cardio in a gym setting. Lower body resistance exercises including squats, leg press, and deadlifts remain restricted until 10-12 weeks post-surgery. Always confirm gym readiness with your surgeon at your 6-week follow-up before resuming any structured training programme.
What happens if you exercise too soon after BBL?
Exercising too soon after BBL compresses fat grafts before vascularisation, reducing volume and altering contour. Clinical experience consistently identifies premature activity as one of the leading causes of suboptimal BBL results. Patients who exercise too early may require revision surgery to restore volume lost during the critical fat-integration window.
How do I maintain my BBL results with exercise?
Long-term BBL maintenance requires stable body weight, glute-building resistance training, and consistent calorie intake. Published research shows that patients exercising regularly retain better BBL volume at 3 years. Prioritise glute isolation exercises such as hip thrusts, kickbacks, and step-ups once cleared at 10-12 weeks.
When can I fly after BBL surgery?
Most surgeons permit flying 2-3 weeks after BBL for short-haul and 3-4 weeks for long-haul travel. Standard DVT prevention guidance recommends compression stockings and hourly in-flight movement for all post-operative patients. UK and US patients returning from Istanbul should plan a minimum 3-week stay to receive fly clearance safely.
How long does BBL recovery take in total?
Full BBL recovery, including final fat stabilisation and visible results, takes approximately 6 months in total. Published research indicates, approximately 60% of transferred fat cells establish permanent blood supply by 3 months. Most patients return to full daily activity, including gym workouts and normal sitting, by 10-12 weeks post-operatively.
Conclusion
BBL exercise recovery is a 12-week progression from walking to full training. Respect the fat graft survival window, maintain weight stability, and follow surgeon-specific clearance for lasting results.
The path from day-1 walking to full gym activity after a BBL is structured and evidence-based. The 12-week timeline exists because fat grafts require a stable vascular environment — not because of general surgical caution. Clinical evidence consistently shows that patients who follow phased return-to-exercise protocols retain meaningfully more transferred fat volume than those who resume activity early.
The 5 factors most likely to affect your individual timeline are procedure complexity, age, transfer volume, compression garment compliance, and nutrition during recovery. Of these, compression compliance and calorie intake are the two variables entirely within your control.
For patients travelling from the UK or USA to Carely Clinic Istanbul, the BBL recovery package includes a personalised exercise timeline at discharge, WhatsApp access to your surgeon throughout recovery, and documentation for your GP or primary care doctor.
Individual outcomes vary. This guide provides general medical education based on international guidelines and published research. Consult qualified medical professionals for personalised advice.
Medical Review: Op. Dr. Alirza Jahangirov