
Quick Summary:
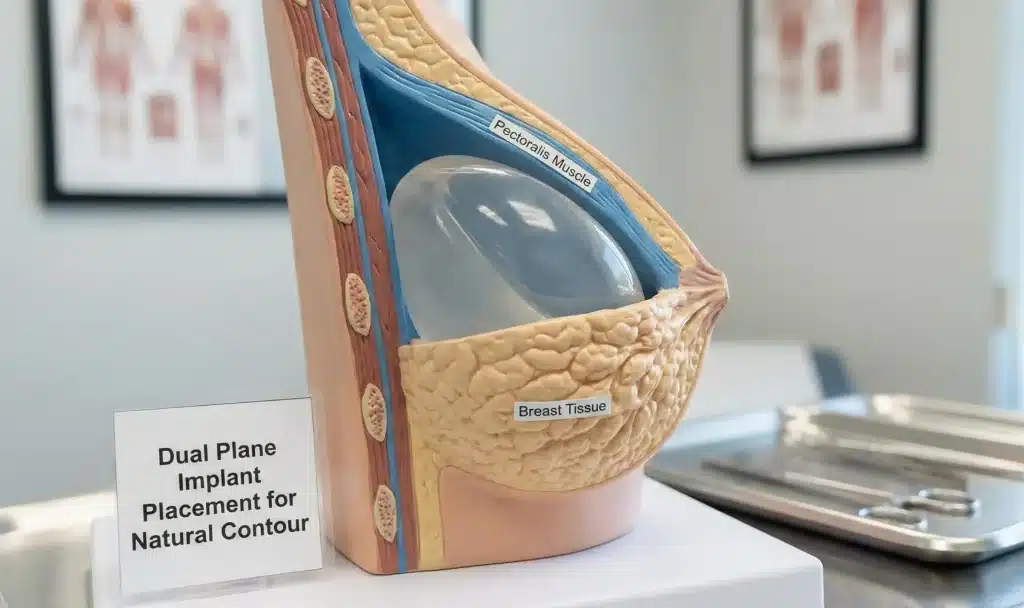
Dual plane breast augmentation positions the implant partially under the pectoralis muscle (upper pole) and partially under breast tissue (lower pole). First described by Dr. John Tebbetts in 2001, it combines the coverage benefits of submuscular placement with the natural lower-pole shaping of subglandular.
ISAPS data shows Turkey performed 48,179 breast augmentations in 2024, with dual plane among the most frequently used techniques at high-volume Istanbul centres. This guide covers the technique, three subtypes, candidacy, risks, and recovery.
Quick Comparison:
| Factor | Dual Plane | Full Submuscular | Subglandular |
|---|---|---|---|
| Upper-pole coverage | ✅ Muscle | ✅ Full muscle | ❌ Tissue only |
| Lower-pole shaping | ✅ Natural fill | ⚠️ Restricted | ✅ Unrestricted |
| Animation deformity risk | ⚠️ Moderate (20–53%) | ⚠️ Higher (58% median) | ✅ None |
| Capsular contracture risk | ✅ Lower | ✅ Lower | ⚠️ Higher |
| Suitable for mild ptosis | ✅ Yes | ⚠️ Partially | ⚠️ Partially |
| Recovery time | 4–6 weeks full | 4–6 weeks full | 2–4 weeks full |
| Rippling risk (thin patients) | ✅ Low | ✅ Low | ⚠️ Higher |
Why Trust This Guide
This guide draws on the original Tebbetts dual plane technique paper (Plastic and Reconstructive Surgery, 2001), a 2024 peer-reviewed study in Aesthetic Surgery Journal Open Forum on animation deformity outcomes, 2025 ISAPS global procedure data, and ASPS clinical guidelines on implant placement.
Carely Clinic’s editorial team reviews all content for accuracy and updates articles when major clinical evidence changes. This is medical education content — not a substitute for a personalized surgical consultation.
What Is Dual Plane Breast Augmentation?
Dual plane breast augmentation places the upper portion of the implant beneath the pectoralis major muscle and the lower portion under breast tissue — combining two anatomical planes to optimize both coverage and shaping simultaneously.
The technique was first formally described by Dallas plastic surgeon Dr. John Tebbetts in a landmark 2001 paper in Plastic and Reconstructive Surgery, where he outlined how selectively releasing the lower muscle origin could solve shaping challenges that neither submuscular nor subglandular placement addressed alone.
To understand why this matters, consider the layered anatomy of the breast: ribs sit at the base, then the pectoralis muscle, then breast tissue and fat, then skin. Traditional submuscular placement positions the entire implant behind the muscle — excellent coverage, but it restricts how the lower breast fills out. Subglandular placement (over the muscle) allows free lower-pole expansion but leaves the implant’s upper edge covered only by thin breast tissue, increasing visible rippling risk in slim patients.
Dual plane resolves this by releasing the lower pectoralis attachment from the chest wall, allowing the muscle to migrate upward while the implant contacts the lower breast tissue directly. The upper implant remains under the muscle; the lower implant is free to shape the breast naturally.
Expert Insight
“Dual plane augmentation adjusts implant–tissue relationships to ensure adequate soft-tissue coverage while optimizing implant dynamics, offering increased benefits and fewer tradeoffs compared with a single pocket location across a wide range of breast types.”
— Tebbetts JB, Plastic and Reconstructive Surgery, 2001 (original technique description, updated in 2006)
How Dual Plane Compares to Other Placement Methods
The three primary placement options — submuscular, subglandular, and dual plane — each suit different anatomy, tissue thickness, and goals, with no single technique universally superior to the others.
Submuscular (full under-muscle) placement covers the implant entirely beneath the pectoralis. It provides maximum soft-tissue protection for thin patients and lowers capsular contracture risk, but restricts lower-pole expansion and carries the highest animation deformity risk because the intact muscle sits over the entire implant.
Subglandular (over-muscle) placement positions the implant above the pectoralis and beneath the breast tissue. Recovery is faster, there is no animation risk, and lower-pole shaping is unrestricted. However, capsular contracture rates are higher and visible rippling or implant edges are a concern in patients with minimal natural breast tissue.
Dual plane sits between these extremes. By partially releasing the lower pectoralis while preserving upper-pole muscle coverage, it delivers the natural look of submuscular placement at the top with the unrestricted lower shaping of subglandular placement. The trade-off is moderate animation deformity risk and a longer recovery than subglandular alone.
For most patients with thin tissue and mild ptosis seeking a natural result, dual plane is the default recommendation at high-volume accredited centres. For athletic women with moderate breast tissue and no ptosis, subglandular or subfascial placement may be discussed. The right choice depends on tissue thickness, ptosis grade, lifestyle, and implant size — all assessed at consultation.
The Three Types of Dual Plane Technique
Dual plane augmentation is not a single operation — it comes in three variations based on how extensively the pectoralis muscle and overlying breast tissue are released. Each type suits a different breast shape and degree of ptosis.
Type I: Minimal Muscle Release
Type I releases only the lower pectoralis origin without separating the breast tissue from the muscle above, preserving the most muscle coverage. It is used for patients with a tight lower-pole envelope, minimal natural tissue, and no sagging.
This is the foundational version of the technique. The muscle still covers a significant portion of the upper and mid-implant, making Type I the closest variant to full submuscular placement in terms of upper-pole coverage. Results tend to be predictable and anatomically contoured, with a natural slope rather than dramatic fullness.
Type II: Moderate Release
Type II additionally separates the breast-muscle interface up to the lower areola border, allowing the implant to expand the lower pole more freely. It is appropriate for patients with mild ptosis, a slightly lower breast fold, or minor soft-tissue laxity.
The moderate release creates more natural inferior fullness while preserving upper muscle support. This is the most commonly performed dual plane variant for post-pregnancy breast deflation with Grade I ptosis, where the lower breast has lost volume but drooping is not severe.
Type III: Maximum Release
Type III releases the breast-muscle attachment up to the nipple level, providing the greatest lower-pole expansion. It is reserved for tuberous breasts, constricted lower poles, or Grade II ptosis requiring implant-driven reshaping.
With the tissue released higher, the implant has maximum freedom to fill and shape the inferior breast. This version produces the most significant lift effect from the implant alone and is often used when the surgeon wants to avoid combining a formal mastopexy with augmentation for borderline cases.
Expert Insight
“Type selection in dual plane augmentation should match the patient’s breast envelope characteristics — tight, normal, or excessively compliant. Applying the wrong type for a breast’s tissue characteristics is the most common technical error.”
— Adapted from Tebbetts JB, Plastic and Reconstructive Surgery, 2006 update on dual plane techniques
Who Is a Good Candidate for Dual Plane?
Dual plane is suited to patients with specific anatomical characteristics and goals — it is not the right choice for everyone, and candidacy depends on tissue thickness, ptosis grade, and lifestyle factors.
Ideal Candidates
Ideal candidates have minimal breast tissue (thin patients where full submuscular would restrict lower-pole shaping), mild to moderate sagging (Grade I–II ptosis), or constricted and tuberous breast deformities needing lower-pole expansion.
Women who have lost breast volume after pregnancy, weight loss, or significant BMI changes are frequent dual plane candidates. The technique fills the deflated lower pole while maintaining the upper-pole coverage that makes results look natural in thin patients. Patients hoping to avoid a breast lift for mild drooping may also be candidates for Type II or III, which can slightly elevate the nipple-areola position.
Who Should Avoid Dual Plane
Patients with severe ptosis (Grade III — nipple significantly below the breast fold) require a formal mastopexy and are not suitable for dual plane alone.
Highly athletic women who perform frequent heavy chest pressing may also wish to discuss subglandular or subfascial placement, given that repeated pectoralis contraction against an implant can — over years — contribute to implant displacement or persistent animation deformity. Women with adequate breast tissue coverage may not need the muscle protection that dual plane provides, making a simpler subglandular approach worth discussing.
For patients interested in dual plane augmentation in Turkey, Carely Clinic’s surgeons assess candidacy using pre-operative photos, breast measurements, and ptosis grading before recommending a technique. See our breast augmentation consultation page for details on the pre-operative assessment process.
Benefits of Dual Plane Breast Augmentation
Dual plane delivers distinct advantages over both single-plane alternatives by optimizing the implant’s interaction with muscle and breast tissue simultaneously — producing results that neither technique achieves alone.
Natural-looking upper pole. Because the pectoralis muscle covers the top of the implant, there is a smooth, gradual transition from the chest to the breast — avoiding the abrupt “shelf” or visible implant edge that can appear with subglandular placement in thin patients.
Lower-pole fullness and shape. With the lower muscle released, the implant contacts the inferior breast tissue directly and helps fill out deflated or constricted lower poles. This produces the teardrop-like inferior fullness that many patients describe as their primary aesthetic goal.
Reduced capsular contracture risk. Partial submuscular placement lowers the risk of capsular contracture (hardening of scar tissue around the implant) compared to subglandular placement. Studies show subglandular placement can increase capsular contracture risk by more than double compared to submuscular techniques.
Mild internal lift effect. Type II and III releases can elevate the nipple-areola position slightly, providing a subtle “internal lift” without the visible scarring of a formal mastopexy. About 17% of dual plane procedures specifically incorporate breast tissue release for this lifting effect, according to published technique data.
Breastfeeding compatibility. The dual plane approach is designed to minimize disruption to milk ducts, nerves, and glandular tissue. Many surgeons report patients successfully breastfeeding after dual plane augmentation, though outcomes vary and cannot be guaranteed.
Longer implant stability. The muscle anchor at the upper pole helps hold the implant in position over time, reducing the rate of inferior implant migration compared to subglandular placement, where the implant has no superior anchor.
Risks and Limitations to Know
Like all breast augmentation techniques, dual plane carries procedural risks as well as specific limitations related to its muscle involvement — and patients should understand both before proceeding.
Animation Deformity
Animation deformity (BAD — breast animation deformity) is the most reported dual plane-specific concern, where the breast visibly distorts or moves during pectoral muscle contraction. A 2024 systematic review found the median BAD incidence across submuscular techniques was 58%, with dual plane reducing — but not eliminating — this risk compared to full submuscular placement.
Persistent animation deformity affects approximately 20% of dual plane patients during exercise, according to published data. For most patients the movement is mild and only visible during intense chest exercises. However, patients who perform frequent chest press, pec fly, or competitive fitness routines should discuss this risk specifically at consultation, as it may influence the placement decision.
Capsular Contracture Risk
Capsular contracture — hardening of the scar capsule around the implant — occurs at rates of 2–4% at accredited centres with dual plane placement, significantly lower than subglandular rates. The partial muscle cover provides a vascularized layer over the implant that reduces the inflammatory environment associated with contracture formation.
Surgeons at accredited facilities use smooth-surface implants and no-touch techniques to further minimize this risk. At Carely Clinic’s partner JCI-accredited Istanbul hospitals, all implants are placed using triple-antibiotic irrigation protocols as standard.
Other procedural risks shared with all breast augmentation techniques include hematoma (2–4%), infection (<1–2% at accredited facilities), implant malposition, wound-healing complications, and altered nipple sensation. A 2025 study in Plastic and Reconstructive Surgery on 178 dual plane patients reported 1 hematoma, 2 cases of grade III/IV capsular contracture, and 5 cases of implant malposition across the cohort.
Recovery Timeline After Dual Plane Surgery
Recovery from dual plane augmentation follows a predictable staged progression driven by the partial muscle release, with full results typically visible at 5–6 months when the implants settle into final position.
Return to Work
Most patients return to desk-based or sedentary work within 5–7 days, with discomfort manageable on oral analgesia. Initial chest tightness is typical as the muscle heals around the implant.
Swelling peaks in the first 2 weeks and gradually subsides over 4–6 weeks. Patients are typically instructed to wear a supportive surgical bra continuously for the first 4–6 weeks. Driving is usually restricted for 1–2 weeks while arm range of motion is limited.
Return to Exercise
Light cardiovascular exercise such as walking can usually resume at 2–3 weeks post-surgery, provided no pectoral engagement is required. Upper-body exercise, chest press, and pec fly should be avoided for 6–12 weeks to prevent displacement of the settling implant and to allow the partial muscle release to heal fully.
Implants begin descending from their initially high position at 3–4 weeks, reaching their final settled shape by 5–6 months. This “drop and fluff” process occurs more predictably after dual plane than after full submuscular placement, because the muscle’s lower tension allows the implant to settle more naturally.
Patients returning to Turkey for follow-up should plan a minimum 7-night stay. Carely Clinic provides remote follow-up via WhatsApp and video consultation for international patients who have returned home before their implants fully settle.
Dual Plane Breast Augmentation Cost by Country
Dual plane breast augmentation cost varies significantly by country, with Turkey offering all-inclusive packages at 55–70% less than equivalent procedures in the UK or USA — without compromising implant quality or surgical accreditation standards.
| Country | Typical Cost Range | What’s Usually Included |
|---|---|---|
| Turkey (Istanbul) | €3,500–€5,500 all-inclusive | Surgery, implants, hospital, anaesthesia, hotel, transfers, follow-up |
| United Kingdom | £5,500–£9,000 | Surgery and hospital; hotel/travel extra |
| United States | $7,000–$12,000 | Surgery and anaesthesia; facility fees often separate |
| Australia | AUD $12,000–$18,000 | Variable; hospital facility fees usually extra |
| Germany | €7,000–€12,000 | Surgery; accommodation and transfers separate |
The lower cost in Turkey is driven by significantly reduced hospital operating costs, lower labour overheads, and favourable exchange rates — not by differences in implant quality or surgical standards. Premium implant brands (Mentor, Motiva, Natrelle) used in Turkey are the same FDA-approved and CE-marked devices used in the UK and USA.
The dual plane technique itself does not add meaningfully to cost compared to standard submuscular placement at the same clinic, as the additional surgical steps (muscle release, tissue dissection) are within the standard operating time for experienced breast surgeons.
How This Applies in Turkey
Turkey performed 48,179 breast augmentations in 2024 per ISAPS data, making it a top-five global destination — with Istanbul surgeons highly experienced in dual plane technique across JCI-accredited facilities.
Turkey ranks among the top five countries globally for breast augmentation volume by total procedures, according to the 2024 ISAPS Global Survey. Istanbul is the primary hub, housing the majority of Turkey’s JCI-accredited private hospitals and the highest concentration of surgeons holding Turkish Board certification in Plastic, Reconstructive, and Aesthetic Surgery (TSPRAS), with many also holding EBOPRAS (European Board) accreditation.
Breast augmentation packages in Istanbul typically range from €3,500 to €5,500 all-inclusive, covering surgery at a JCI-accredited hospital, premium implants, anaesthesia, 1–2 nights’ hospital stay, 5–7 nights’ hotel accommodation, airport transfers, and post-operative care. This compares to £5,500–£9,000 in the UK for surgery only.
At Carely Clinic, our breast augmentation surgeons are TSPRAS board-certified and perform dual plane augmentation routinely, with extensive experience across Type I, II, and III techniques. Pre-operative assessment — including ptosis grading and tissue thickness measurement — is conducted on arrival day, so international patients complete all testing and consultation in a single day before surgery the following morning.
Our follow-up protocol for international patients includes in-person review before departure and remote check-ins at 2 weeks, 6 weeks, and 6 months via our patient coordination team. Patients receive implant documentation, surgical summary records, and emergency contact information for use with their home physician if needed.
Learn more about breast augmentation at Carely Clinic or contact our team to request a consultation and package quote.
Dual Plane vs. Alternatives: Quick Comparison Table
Dual plane, full submuscular, and subglandular placement each carry distinct advantages — this table summarises the key clinical differences to support an informed conversation with your surgeon.
| Factor | Dual Plane | Full Submuscular | Subglandular | Subfascial |
|---|---|---|---|---|
| Best for | Thin patients, mild ptosis, deflation | Very thin patients, reconstruction | Athletic women, good tissue coverage | Active women wanting no animation risk |
| Animation deformity | Moderate (20–53%) | Higher (58% median) | None | None |
| Capsular contracture risk | Lower (2–4%) | Lower (2–4%) | Higher (>2x) | Intermediate |
| Ptosis correction ability | Mild–moderate (Grade I–II) | Minimal | Minimal | Minimal |
| Mammography clarity | Good | Good | Reduced | Reduced |
| Full recovery | 5–6 months | 5–6 months | 3–4 months | 3–4 months |
To explore which placement technique is right for your anatomy, visit our breast augmentation guide or review our round vs. teardrop implant comparison for related implant decisions.
Frequently Asked Questions
What is dual plane breast augmentation?
Dual plane breast augmentation is a surgical technique where the upper portion of the implant sits beneath the pectoralis muscle and the lower portion rests under breast tissue, first described by Dr. John Tebbetts in Plastic and Reconstructive Surgery in 2001. This hybrid pocket combines the natural coverage of submuscular placement at the top with the full lower-pole shaping of subglandular placement below. The result is a smoother upper-pole transition, reduced implant visibility in thin patients, and better lower-breast contour than either single-plane method alone.
What is the difference between dual plane and submuscular breast augmentation?
In fully submuscular placement, the entire implant sits beneath the pectoralis muscle, while in dual plane the lower muscle origin is partially released so only the upper implant is covered by muscle. Full submuscular placement offers maximum coverage but restricts lower-pole expansion and increases the risk of animation deformity compared to dual plane. Dual plane reduces muscle tension on the lower implant, allowing more natural inferior fullness while preserving upper-pole coverage for thinner patients.
Who is a good candidate for dual plane breast augmentation?
Ideal candidates are women with minimal natural breast tissue seeking a natural look, those with mild to moderate breast sagging (ptosis Grade I–II), and patients with constricted or tuberous lower poles who need implant-driven expansion. Women with significant sagging (Grade III ptosis) typically require a mastopexy rather than dual plane alone, as the technique cannot adequately address severe drooping. Athletic women and those who want to avoid full muscle division often benefit from dual plane’s partial release approach.
What are the disadvantages of dual plane breast augmentation?
The primary disadvantage is animation deformity — visible implant movement or distortion during pectoral contraction — which affects approximately 20–53% of dual plane patients to some degree according to published data. Recovery is longer than subglandular placement because the partial muscle release requires additional healing time, with most surgeons advising 6–12 weeks before resuming upper-body exercise. The technique is also more technically demanding than single-plane options, requiring a surgeon experienced in breast anatomy and implant–tissue dynamics.
Does dual plane breast augmentation cause animation deformity?
Yes, animation deformity — where the breast shape visibly distorts during pectoral muscle contraction — can occur with dual plane, but less severely than with full submuscular placement. A systematic review published in PMC found the median BAD (breast animation deformity) rate across submuscular techniques was 58%, while dual plane’s partial release reduces this risk by lessening muscle tension over the implant. Most patients notice mild movement only during intense chest exercises, and for many it is cosmetically acceptable.
How long is recovery after dual plane breast augmentation?
Most patients return to desk work within 5–7 days and resume light cardiovascular activity at 2–3 weeks post-surgery. Upper-body exercise, chest press, and high-impact activities should be avoided for 6–12 weeks to allow the partial muscle release to fully heal and the implants to settle. Implants typically begin descending into final position at 3–4 weeks and reach their fully settled shape by 5–6 months.
Is dual plane better than over-the-muscle placement?
Neither is universally better — the best placement depends on individual anatomy, tissue thickness, and aesthetic goals. Subglandular (over-the-muscle) placement offers faster recovery and no animation risk, but carries a higher rate of capsular contracture and visible rippling, particularly in thin patients. Dual plane is preferred when patients have minimal breast tissue, mild sagging, or constricted lower poles, as it provides coverage where subglandular placement cannot.
Can dual plane breast augmentation replace a breast lift?
Dual plane can provide a mild internal lift effect for patients with Grade I–II ptosis (mild sagging), potentially avoiding a formal mastopexy in borderline cases. However, it is not a substitute for a breast lift in women with moderate to severe ptosis — the implant alone cannot adequately reposition a significantly drooping nipple-areola complex. Surgeons assess ptosis grade at consultation to determine whether dual plane alone, or dual plane combined with mastopexy, is appropriate.
What are the three types of dual plane technique?
Type I involves minimal pectoralis release with no breast tissue separation from muscle, used for patients with tight envelopes and minimal sagging. Type II releases the lower muscle border further and separates breast-muscle attachments to the lower areola border, suitable for mild ptosis and slightly deflated breasts. Type III maximises the muscle and tissue release to the nipple level, used for the greatest degree of lower-pole expansion in patients with tuberous breasts or more significant constriction.
Is dual plane breast augmentation safe?
Dual plane augmentation is considered safe when performed by an experienced, board-certified plastic surgeon at an accredited facility, with overall complication rates comparable to other placement methods. Major complications including capsular contracture, hematoma, and infection occur at rates of 2–4% at accredited centres, according to ASPS data. Animation deformity is the most commonly reported concern specific to dual plane, affecting up to 53% of patients to some degree, though most cases are mild and cosmetically acceptable.
How long do dual plane breast implants last?
Modern cohesive silicone implants placed via dual plane technique have no defined expiration date, but the FDA recommends monitoring every 5–6 years with MRI or ultrasound to detect silent rupture. ASPS data indicates approximately 20% of patients undergo implant revision within 10 years — most commonly for aesthetic preference changes, capsular contracture, or implant exchange rather than safety concerns. Dual plane placement does not inherently shorten or extend implant lifespan compared to other techniques.
Conclusion
Dual plane breast augmentation is a technically advanced hybrid technique offering natural upper-pole coverage and improved lower-pole shaping, with animation deformity affecting approximately 20–53% of patients to some degree.
For the right candidate — thin patients, women with mild ptosis, or those needing lower-pole expansion after pregnancy or weight loss — dual plane delivers results that neither full submuscular nor subglandular placement achieves independently. Type I is suitable for patients with tight envelopes and minimal sagging; Type II and III address progressively greater degrees of ptosis and deflation. Animation deformity is a genuine consideration for very athletic patients and should be discussed at consultation.
If you are researching dual plane augmentation and want to understand whether it is right for your anatomy, Carely Clinic’s surgical team offers pre-operative assessments covering ptosis grading, tissue thickness measurement, and implant-selection guidance. All procedures are performed at JCI-accredited Istanbul hospitals using premium CE-marked and FDA-approved implants.
Individual requirements and outcomes vary. This guide provides general information based on published clinical guidelines and peer-reviewed research. Consult a qualified plastic surgeon for personalized recommendations.
Medical Review: Dr. Alirza Jahangirov