
Quick Summary
Gastric sleeve (VSG) removes 80% of the stomach and produces 60-70% excess weight loss at one year, while gastric bypass (RYGB) creates a small stomach pouch and reroutes the intestine for 70-80% excess weight loss and stronger type 2 diabetes remission rates of up to 80%. Per 2022 ASMBS/IFSO guidelines, both require BMI 40+ or BMI 35+ with a qualifying comorbidity.
In Turkey in 2026, sleeve costs £2,100-£3,600 ($2,600-$4,400) and bypass costs £2,300-£3,900 ($2,750-$4,800). This guide compares both procedures across 7 key decision factors.
What Is the Difference Between Gastric Sleeve and Gastric Bypass?
Gastric sleeve (VSG) and gastric bypass (RYGB) account for 90% of all bariatric procedures worldwide, per 2022 ASMBS/IFSO guidelines. Sleeve removes 80% of the stomach, achieving 60-70% excess weight loss at one year. Bypass creates a small pouch and reroutes the intestine, reaching 70-80% excess weight loss with up to 80% type 2 diabetes remission.
Sleeve is faster (45-90 minutes) and carries fewer long-term nutritional risks. Bypass is better for patients with severe GERD, BMI above 50, or insulin-dependent diabetes, per ASMBS and BOMSS guidance. In Turkey in 2026, sleeve costs £2,100-£3,600 ($2,600-$4,400) and bypass costs £2,300-£3,900 ($2,750-$4,800).
The right choice depends on your BMI, comorbidities, and lifestyle goals — a bariatric consultation is essential.
Why Trust This Guide
This comparison draws on the 2022 ASMBS/IFSO indications guidelines, a 2024 JAMA Network Open randomised clinical trial (the BEST trial, Sweden-Norway), and a 2025 JAMA Surgery population study of 39,067 adults. UK context is informed by British Obesity and Metabolic Surgery Society (BOMSS) published guidance. Assoc. Prof. Dr. Gökmen Öztürk has performed 5,000+ bariatric surgeries over 25 years. This guide provides medical education and does not replace personalised clinical consultation.
How Each Procedure Works: Mechanism and Surgery Details
Two proven procedures, two different mechanisms. Sleeve and bypass both reduce how much you eat, but bypass goes further by changing how your body absorbs nutrients. Understanding the mechanism helps you understand every other difference in this guide.
Gastric Sleeve (VSG): How It Works
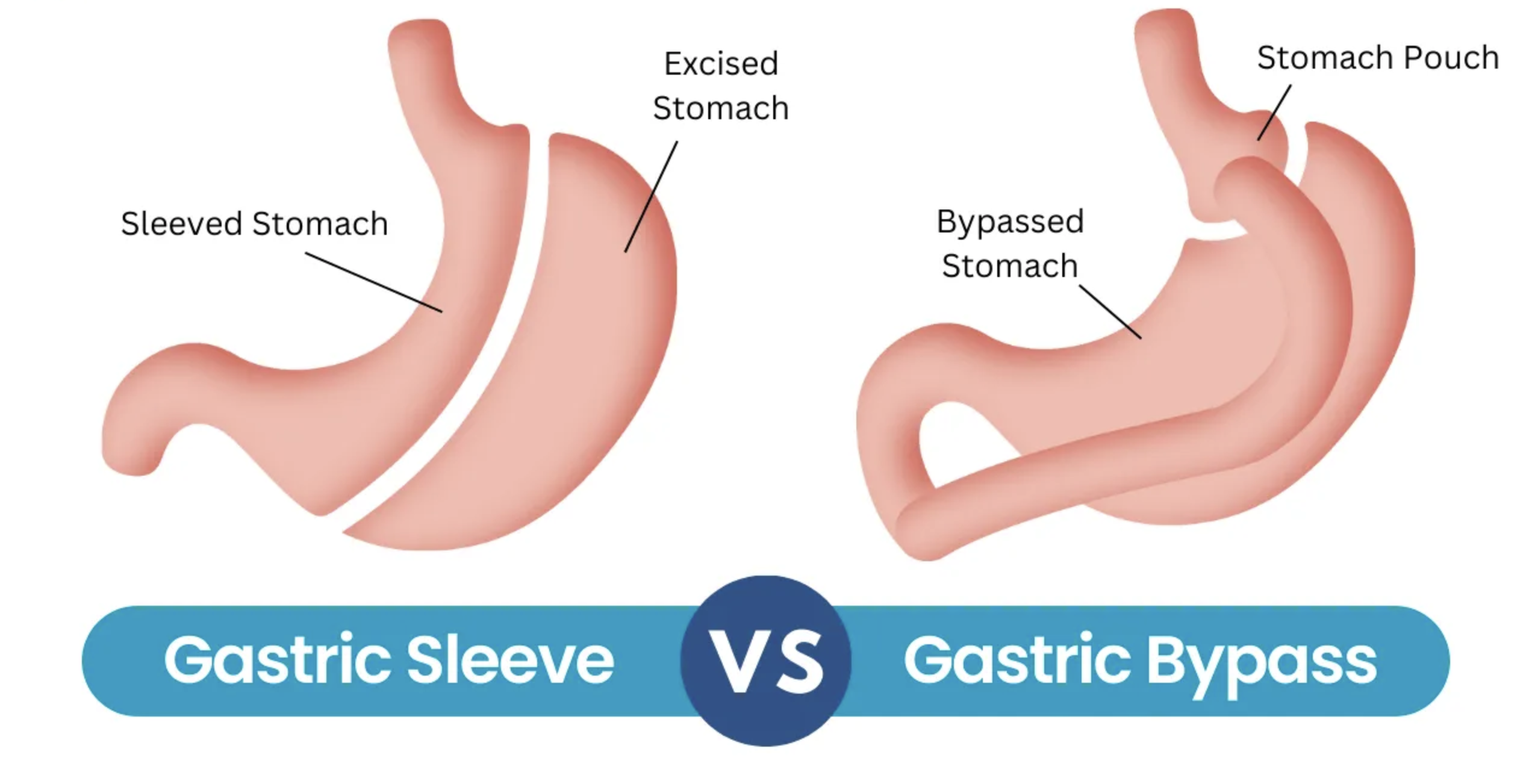
Restriction plus hunger hormone reduction. Sleeve removes approximately 80% of the stomach laparoscopically, leaving a narrow, banana-shaped tube. This works through two pathways.
The remaining stomach holds far less food, so you feel full quickly. Crucially, the removed portion includes the fundus — the region producing most of the body’s ghrelin, the primary hunger-signalling hormone. Lower ghrelin means significantly reduced appetite, not just a smaller stomach. Surgery takes 45-90 minutes under general anaesthesia.
Gastric Bypass (Roux-en-Y): How It Works
Restriction plus malabsorption plus metabolic reset. Bypass (Roux-en-Y Gastric Bypass, or RYGB) is a two-part procedure. First, the surgeon staples the upper stomach into a thumb-sized pouch of roughly 15-30ml. Second, the small intestine is divided and reconnected directly to this pouch, bypassing the remaining stomach and the duodenum entirely.
This creates three simultaneous effects: severely restricted food intake, reduced caloric absorption, and an immediate hormonal metabolic shift that improves insulin sensitivity — often within days of surgery. Bypass takes 2-3 hours under general anaesthesia.
| Feature | Gastric Sleeve (VSG) | Gastric Bypass (RYGB) |
|---|---|---|
| What it does | Removes ~80% of stomach | Small pouch + intestinal rerouting |
| Mechanism | Restrictive only | Restrictive + malabsorptive |
| Surgery duration | 45-90 minutes | 2-3 hours |
| Hospital stay | 2-3 nights | 3-4 nights |
| Excess weight loss (1 yr) | 60-70% | 70-80% |
| Type 2 diabetes remission | ~60% | ~80% |
| Effect on GERD | Can worsen (~20% of patients) | Usually resolves |
| Reversible | No | Technically yes, rarely performed |
| Vitamin burden | Daily, long-term | Lifelong + B12, calcium citrate, iron |
| Cost in Turkey (2026) | £2,100-£3,600 / $2,600-$4,400 | £2,300-£3,900 / $2,750-$4,800 |
7 Key Factors That Determine Which Surgery Is Right for You
No single procedure is universally superior. The right choice comes down to seven specific clinical factors your bariatric surgeon will assess during your pre-operative workup. Here is what each factor means for your decision.
Factor 1: BMI and Starting Weight
Bypass produces greater results above BMI 50. For patients with BMI 35-45, sleeve delivers comparable outcomes at lower risk. Per Denver Health Bariatric Surgery Center guidelines and ASMBS 2022 updated indications, patients with BMI above 50 generally achieve measurably greater weight loss with bypass than with sleeve.
Factor 2: Type 2 Diabetes and Metabolic Disease
Bypass is the metabolic intervention of choice for uncontrolled diabetes. Randomised clinical trials cited in ASMBS guidance show bypass produces insulin sensitivity improvements within days — before significant weight loss occurs. For patients on insulin with poor HbA1c control, bypass produces approximately 80% diabetes remission versus 60% for sleeve.
Factor 3: GERD and Acid Reflux
Sleeve can worsen reflux; bypass reliably resolves it. Approximately 20% of sleeve patients experience worsening GERD post-operatively due to increased intragastric pressure. Bypass reroutes food away from the lower oesophageal sphincter entirely, resolving reflux symptoms in most patients. Patients with confirmed Barrett’s oesophagus should not undergo sleeve, per ASMBS 2022 indications guidance.
Factor 4: Long-Term Nutrition and Supplement Burden
Bypass patients carry a heavier lifelong supplement commitment. Because bypass bypasses the duodenum — the primary site of iron, calcium, and vitamin B12 absorption — deficiencies develop without strict supplementation. Sleeve patients must also supplement, but the pathway is simpler and deficiencies are less severe. Both procedures require annual blood work, per BOMSS 2023 post-operative care recommendations.
Factor 5: Surgery Complexity and Anaesthetic Risk
Sleeve is the lower-risk option for complex patients. Sleeve takes 45-90 minutes under anaesthesia versus 2-3 hours for bypass. For patients with significant cardiac or pulmonary comorbidities, shorter anaesthetic duration reduces perioperative risk. Your surgical team will assess your anaesthetic risk score during pre-operative screening.
Factor 6: Weight Loss Volume and Speed
Bypass produces faster and greater total weight loss. ASMBS 2025 data confirm bypass patients maintain 70-75% excess weight loss at five years versus 60-65% for sleeve. Additionally, a 2025 JAMA Surgery population-based cohort study of 39,067 adults found bypass was associated with a lower risk of major adverse cardiac events (MACE), including reduced myocardial infarction rates, compared with sleeve over up to 11 years of follow-up.
Factor 7: Reversibility and Future Surgical Options
Sleeve is irreversible; bypass is technically reversible but rarely reversed. Once 80% of the stomach is removed in a sleeve, it cannot be restored. Bypass can technically be reversed but this is rarely performed due to complexity and risk. However, sleeve can be converted to bypass — a useful option if GERD worsens or weight loss stalls, with BOMSS 2023 guidance recommending at least 18-24 months before conversion is considered.
Expert Insight
“In a 2025 head-to-head study presented at the ASMBS Annual Scientific Meeting, sleeve gastrectomy and gastric bypass were associated with approximately five times more excess weight loss than GLP-1 receptor agonists (semaglutide or tirzepatide) at two years. Surgery remains the most durable intervention for severe obesity when long-term outcomes are the measure.”
— American Society for Metabolic and Bariatric Surgery (ASMBS), 2025
Weight Loss Results: What the Clinical Evidence Shows
Clinical evidence consistently favours bypass for total weight loss volume — but sleeve is far from inferior. A 2024 JAMA Network Open randomised clinical trial (the BEST trial, Sweden and Norway) confirmed bypass carries slightly higher short-term surgical risk while producing greater weight loss and stronger metabolic outcomes.
For most patients with BMI 35-45 seeking significant weight loss without maximum metabolic intervention, sleeve achieves 60-70% excess weight loss within 12-18 months and represents an excellent risk-benefit profile. For patients where the additional 10-15% excess weight loss matters clinically — those with severe diabetes, BMI above 50, or cardiovascular risk factors — bypass delivers meaningfully better long-term outcomes.
Both bariatric procedures dramatically outperform medical management and lifestyle intervention alone for sustained weight loss at five years.
Risks and Complications: Sleeve vs Bypass Safety Data
Every bariatric surgery carries risk. Sleeve has a complication rate below 1% for major surgical events. Bypass is more complex and carries a slightly higher short-term surgical risk, although long-term metabolic benefits often outweigh this for appropriate candidates.
Per the 2024 BEST randomised trial (JAMA Network Open, Hedberg et al.), both procedures have well-characterised safety profiles, with bypass associated with higher rates of nutritional deficiency and sleeve with higher rates of long-term GERD. The 2025 JAMA Surgery cohort study of 39,067 adults found bypass associated with lower major adverse cardiac events over 11 years — a cardiovascular advantage no competitor Turkey article currently addresses.
Specific risks to discuss with your surgeon include, for sleeve: staple line leak (0.1-1%), GERD worsening, and weight regain after five years. For bypass: internal hernia (1-3%), dumping syndrome (15-20% of patients), marginal ulcer, and lifelong B12, iron, and calcium citrate supplementation requirements.
Warning Signs to Watch For After Bariatric Surgery
Both procedures require the same post-operative vigilance. Most complications appear in the first 30 days. Knowing when to contact your surgeon or seek emergency care can be lifesaving. International patients returning home should share this table with their GP or primary care doctor immediately after travel.
| Warning Sign | What It May Indicate | Action Required |
|---|---|---|
| Fever above 38.5°C (101.3°F) | Infection, anastomotic leak, abscess | Contact surgeon immediately; go to A&E if temperature rises further |
| Sudden or worsening abdominal pain | Staple line leak, internal hernia (bypass), bowel obstruction | Go to emergency department immediately; do not wait |
| Wound separation or discharge | Wound infection, dehiscence | Contact your GP or bariatric team within 24 hours |
| Calf pain, swelling, or redness | Deep vein thrombosis (DVT) | Go to A&E / ER immediately; may indicate clot requiring anticoagulation |
| Shortness of breath or chest pain | Pulmonary embolism, cardiac event | Call 999 (UK) / 911 (US) immediately; this is a medical emergency |
| Persistent vomiting or inability to swallow | Stricture, anastomotic narrowing, obstruction | Contact bariatric surgeon within 24 hours; may need endoscopic dilation |
| Rapid heart rate, dizziness, sweating after eating | Dumping syndrome (bypass patients primarily) | Contact bariatric dietitian; dietary adjustment usually resolves this |
Who Is NOT a Good Candidate?
Not every patient who wants bariatric surgery is a safe candidate. A thorough pre-operative assessment — including blood work, cardiac evaluation, and psychological screening — determines whether sleeve or bypass is appropriate, or whether surgery should be deferred or declined.
Absolute Contraindications
These conditions prevent both procedures from being safely performed.
- Active malignancy: Patients undergoing treatment for cancer cannot safely undergo elective bariatric surgery. Surgery may be reconsidered after confirmed remission and oncologist clearance.
- Severe, uncontrolled psychiatric illness: Untreated psychosis, active eating disorders including binge eating disorder, and severe untreated depression are absolute contraindications. Per ASMBS 2022 guidelines, psychological clearance is a pre-operative requirement.
- Active substance dependence: Alcohol or drug dependence within the preceding 12 months is an absolute contraindication to both procedures, due to risk of transfer addiction and non-compliance post-operatively.
- Barrett’s oesophagus: Patients with Barrett’s oesophagus should not undergo gastric sleeve. Bypass may be considered on a case-by-case basis with specialist gastroenterology review.
- Inability to comply with post-operative requirements: Patients who cannot commit to lifelong supplementation, dietary changes, and follow-up appointments are not suitable candidates for either procedure.
Relative Contraindications
These conditions may allow surgery after optimisation.
- Uncontrolled type 2 diabetes (HbA1c above 10%): Surgery can proceed after a period of medical optimisation to reduce surgical and anaesthetic risk. Bypass is typically preferred over sleeve in this group.
- Severe GERD with hiatal hernia: Sleeve is contraindicated; bypass with concurrent hiatal hernia repair may be appropriate. Full upper GI endoscopy is required pre-operatively.
- BMI below 35: Both ASMBS (US) and BOMSS (UK) guidelines require BMI 35+ with a qualifying comorbidity, or BMI 40+ without. Lower BMI patients may qualify only where metabolic disease is severe and documented.
- Prior complex abdominal surgery: Dense adhesions from previous surgeries increase laparoscopic complexity. Your surgeon will assess feasibility on a case-by-case basis.
Managing Expectations
Surgery is a tool, not a cure. Both sleeve and bypass require permanent lifestyle change — high-protein diet, regular exercise, and consistent supplement compliance — to achieve and maintain long-term results. Weight regain is possible with either procedure if dietary habits are not sustained. Most patients reach their lowest weight 12-18 months post-surgery, with long-term success defined by sustaining 50% or more excess weight loss at five years.
Based on Assoc. Prof. Dr. Gökmen Öztürk’s clinical experience across more than 5,000 bariatric cases, the patients who achieve the best long-term outcomes are those who engage with dietary counselling before surgery and maintain regular follow-up appointments in the first 24 months post-operatively — regardless of whether they chose sleeve or bypass.
Recovery Timeline: What to Expect Week by Week
Recovery from sleeve is faster, but both procedures follow the same dietary progression. Here is what patients typically experience.
Hospital stays run 2-3 nights for sleeve and 3-4 nights for bypass, followed by a 4-6 week progression from liquids to soft foods to regular meals. Sleeve patients return to light activity within 2-3 weeks; bypass patients typically need 4-6 weeks for comparable recovery. Full return to unrestricted exercise takes 3-6 months for both procedures.
| Timeframe | Gastric Sleeve | Gastric Bypass |
|---|---|---|
| Days 1-3 | Hospital, clear liquids, walking encouraged | Hospital, clear liquids, pain managed with IV |
| Week 1-2 | Full liquids at home; rest; short walks | Full liquids; rest; fatigue common |
| Weeks 3-4 | Pureed foods; return to desk work | Pureed foods; rest still recommended |
| Weeks 5-6 | Soft foods; light exercise permitted | Soft foods; return to light work |
| Months 3-6 | Regular foods; full exercise | Regular foods; full exercise |
| 12-18 months | Maximum weight loss typically reached | Maximum weight loss typically reached |
ASMBS follow-up protocol recommends clinical review at 3, 6, and 12 months post-surgery, then annually. Carely Clinic provides lifetime remote follow-up for all international patients, including UK and US patients returning home after their Istanbul procedure.
How This Applies in Turkey
Turkey performs over 50,000 bariatric procedures annually, ranking among Europe’s highest-volume destinations per IFSO 2024 data, with costs 60-70% below UK and US private prices.
Turkey’s position in global bariatric surgery. Turkey has become one of the most active bariatric surgery destinations for patients from the UK, US, and across Europe. Per IFSO 2024 registry data, Turkey ranks among the top five European nations by bariatric procedure volume. Surgeons train under a structured academic and residency pathway at university hospitals, with senior bariatric surgeons commonly holding Associate Professor or Professor titles alongside clinical roles. JCI-accredited hospital facilities are standard for medical tourism clinics accepting international patients.
Cost comparison. In Turkey in 2026, all-inclusive bariatric packages typically cover surgery, anaesthesia, hospital accommodation, pre-operative tests, post-operative medication, airport transfers, and hotel accommodation during recovery. Gastric sleeve packages run approximately £2,100-£3,600 ($2,600-$4,400 / €2,500-€4,200). Gastric bypass packages run approximately £2,300-£3,900 ($2,750-$4,800 / €2,700-€4,600). UK private hospital prices for the same procedures typically run £8,000-£15,000, making Turkey 60-70% less expensive. Explore weight loss surgery packages at Carely Clinic for current inclusions.
Carely Clinic specifically. Assoc. Prof. Dr. Gökmen Öztürk leads bariatric surgery at Carely Clinic in Istanbul. He holds an Associate Professorship, trained at Uludağ University Faculty of Medicine, and has performed 5,000+ procedures across 47 countries of patient origin. His laparoscopic approach — applying techniques he pioneered in Turkey from 2002 — minimises hospital stay and recovery time for both sleeve and bypass patients. Learn more about gastric sleeve surgery at Carely Clinic and gastric bypass surgery at Carely Clinic.
When Can You Fly After Surgery?
Most sleeve patients are cleared to fly 7-10 days post-surgery; bypass patients typically wait 10-14 days. DVT risk is elevated in the early post-operative period, and long-haul flights to the UK or US amplify this risk. Your surgical team will provide written fit-to-fly clearance before discharge.
For flights over 4 hours, wear graduated compression stockings, walk the cabin every 45-60 minutes, and stay well-hydrated with water — not alcohol. Patients on anticoagulant medication should confirm dosing with their surgeon before flying. Share your discharge summary with your GP or primary care doctor within 48 hours of returning home.
Explore all weight loss surgery options at Carely Clinic or review weight loss surgery costs in Turkey for a full price breakdown.
Frequently Asked Questions
Which is safer: gastric sleeve or gastric bypass?
Gastric sleeve carries a complication rate below 1%, making it the simpler and lower-risk procedure. The 2024 BEST trial (JAMA Network Open) found bypass carries slightly higher short-term surgical risk than sleeve. For patients with multiple comorbidities or higher anaesthetic risk, sleeve is generally the surgeon’s safer first choice.
Which surgery results in more weight loss?
Gastric bypass achieves 70-80% excess weight loss at one year versus 60-70% for gastric sleeve. ASMBS 2025 data show bypass patients maintain 70-75% excess weight loss at five years versus 60-65% for sleeve. Patients with higher starting BMI tend to see the greatest additional benefit from choosing bypass over sleeve.
What is the difference between gastric sleeve and gastric bypass?
Sleeve removes 80% of the stomach permanently; bypass creates a small pouch and reroutes the small intestine.Sleeve is purely restrictive, while bypass adds malabsorption, meaning the body absorbs fewer calories from food eaten. Bypass is more complex, lasting 2-3 hours under general anaesthesia versus 45-90 minutes for sleeve surgery.
Who is a better candidate for gastric bypass vs gastric sleeve?
Bypass is strongly preferred for patients with severe GERD, BMI above 50, or insulin-dependent type 2 diabetes.Sleeve suits patients seeking a simpler procedure with lower surgical risk who do not have these specific conditions. A bariatric surgeon determines candidacy after reviewing your BMI, comorbidities, prior abdominal surgeries, and nutrition status.
Does gastric bypass or sleeve work better for type 2 diabetes?
Gastric bypass achieves type 2 diabetes remission in approximately 80% of patients versus 60% for gastric sleeve.Randomised trials cited by ASMBS show bypass produces metabolic improvement within days, before significant weight loss occurs. For patients on insulin with poor HbA1c control, ASMBS guidelines favour bypass as the preferred metabolic intervention.
What are the long-term risks of gastric bypass vs gastric sleeve?
Bypass carries lifelong risks including nutrient deficiencies, internal hernia, and dumping syndrome affecting up to 20% of patients. Sleeve long-term risks include GERD worsening in roughly 20% of patients and potential weight regain after five years. Both procedures require lifelong follow-up with a bariatric team, per BOMSS 2023 post-operative care recommendations.
How long is recovery from gastric bypass compared to gastric sleeve?
Sleeve patients return to light activity within 2-3 weeks; bypass patients typically need 4-6 weeks for comparable recovery. Hospital stays run 2-3 nights for sleeve and 3-4 nights for bypass, followed by 4-6 weeks of dietary progression. Full return to exercise and unrestricted diet takes 3-6 months for both procedures, regardless of which is chosen.
Which procedure is better for GERD or acid reflux?
Bypass is the preferred choice for patients with GERD, as it reliably resolves reflux in the majority of cases. Sleeve can worsen GERD in approximately 20% of patients due to increased intragastric pressure after stomach reduction. Patients with confirmed Barrett’s oesophagus should not undergo sleeve gastrectomy, per ASMBS 2022 updated indications guidance.
Can gastric sleeve be converted to gastric bypass later?
Sleeve can be surgically converted to bypass if significant weight regain or severe GERD develops after the initial procedure. Conversion is more complex than the original sleeve surgery and carries higher surgical risk than a primary bypass procedure. BOMSS 2023 guidance recommends a minimum of 18-24 months post-sleeve before conversion surgery is considered at specialist centres.
How much does gastric bypass vs gastric sleeve cost in Turkey?
In Turkey in 2026, gastric sleeve costs approximately £2,100-£3,600 ($2,600-$4,400 / €2,500-€4,200) all-inclusive.Gastric bypass in Turkey costs approximately £2,300-£3,900 ($2,750-$4,800 / €2,700-€4,600) including hospital stay and transfers. UK private prices for both procedures typically run £8,000-£15,000, making Turkey 60-70% less expensive for equivalent surgery.
Do you need vitamins for life after gastric bypass and gastric sleeve?
Both surgeries require daily supplements, but bypass demands a more complex lifelong regimen due to intestinal malabsorption. Bypass patients must take a bariatric multivitamin, calcium citrate, vitamin D, vitamin B12, and iron supplements indefinitely. Sleeve patients also supplement long-term but generally require fewer vitamins, as nutrient absorption pathways remain intact.
What is dumping syndrome and which surgery causes it?
Dumping syndrome occurs when food passes too quickly into the small intestine, causing nausea, sweating, and rapid heartbeat. It affects 15-20% of gastric bypass patients and is triggered primarily by high-sugar or high-fat foods after surgery. Gastric sleeve rarely causes dumping syndrome, as the intestinal pathway is not altered during the procedure.
Conclusion
Both gastric sleeve and gastric bypass deliver life-changing weight loss. Sleeve suits most patients; bypass is indicated where diabetes control, GERD resolution, or BMI above 50 demand stronger metabolic intervention.
Gastric sleeve is the right choice for the majority of patients: BMI 35-50, no severe GERD, moderate diabetes or no diabetes, and preference for shorter surgery and faster recovery. It achieves 60-70% excess weight loss at one year with a complication profile below 1% and a simpler post-operative supplement regimen.
Gastric bypass delivers greater weight loss (70-80% excess weight loss at one year), stronger type 2 diabetes remission (80%), GERD resolution in most patients, and — per 2025 JAMA Surgery data — a lower long-term risk of major cardiac events. These advantages come with higher surgical complexity, longer recovery, and a lifelong supplement burden.
In Turkey in 2026, both procedures are available at 60-70% below UK and US private prices, without waiting lists. The right starting point is a free consultation with Assoc. Prof. Dr. Gökmen Öztürk to review your specific BMI, comorbidities, and health goals.
Individual outcomes vary. This guide provides general medical education based on international guidelines and published research. Consult qualified medical professionals for personalised advice.
Medical Review: Assoc. Prof. Dr. Gökmen Öztürk